
Of the many ethical dilemmas thrown up by the Covid-19 pandemic, few are greater than the question of vaccinating children.
For many families, this challenge comes centre-stage from next week, with the beginning of registration for 12-15 year olds for administration of the vaccine.
For children with underlying health conditions, there is a clear case for recommending the vaccine, as the risks of Covid-19 infection greatly exceed any posed by taking the vaccine.
But for the broad mass of healthy adolescents, the consideration of whether they should be given a new vaccine under emergency use authorisation, when their risk of serious illness from Covid-19 is minimal, is finely balanced.
This can be seen in the differing policy responses in different countries. France, Israel and Canada, for example, have gone down the route of universal vaccination from 12 years, while the UK and Norway are focusing on vaccinating vulnerable children.
Here, our experts in the National Immunisation Advisory Committee (Niac) have recommended that all those aged 12-15 years "should be offered" an mRNA vaccine (effectively Pfizer as it is the only vaccine authorised for this age group as of now).
In stronger language, children with underlying medical conditions, as well as those living with vulnerable siblings or adults, are being “strongly encouraged” to get vaccinated quickly.
Endorsing Niac's recommendation to Government, chief medical officer Dr Tony Holohan repeated its wording, with the sole change of underlying the word "all" (12-15 year olds).
So while the wording is restrained, and Niac stresses that any decision by parents to accept, refuse or defer vaccination should be respected, the spirit of public policy clearly favours universal vaccination of this age group.
In the UK, the Joint Committee on Vaccination and Immunisation (JCVI) – the equivalent of Niac – advised against routine universal vaccination of children until more data becomes available.
Potential risks
“The health benefits in this population are small, and the benefits to the wider population are highly uncertain,” the JCVI concluded last month.
“At this time, JCVI is of the view that the health benefits of universal vaccination in children and young people below the age of 18 years do not outweigh the potential risks.”
As most people know by now, children are largely spared the ill-effects of Covid-19. Most infections are asymptomatic or mild. Hospitalisation rates are low and deaths rare.
In Ireland, a healthy child has a one in 100,000 risk of ending up in hospital due to Covid-19.
Among all 12-15 year olds, there were 34 admissions in 2020 and 56 so far this year, and no deaths among this group. Fewer than five admissions to paediatric ICU have been linked to Covid-19.
At the start of the pandemic, there was concern over reports of a multisystem inflammatory condition in children, but treatment has improved as awareness of the condition has grown. Up to last February, 32 cases of this condition had been reported in Ireland, with all children recovering successfully.
In any case, as Niac acknowledges, it is not yet known whether vaccination will prevent this condition occurring. In the UK, the JCVI found the available data was insufficient to advise on vaccination to prevent it.
As for “long Covid”, the JCVI said the risk was “very low” while Niac spoke of “considerable uncertainty” around the risk.
Earlier this week, the first large-scale study on Covid and children found most recovered quickly from the disease. Just 1.8 per cent experienced symptoms for longer than eight weeks. Again, the impact of vaccines on long Covid is not yet known.
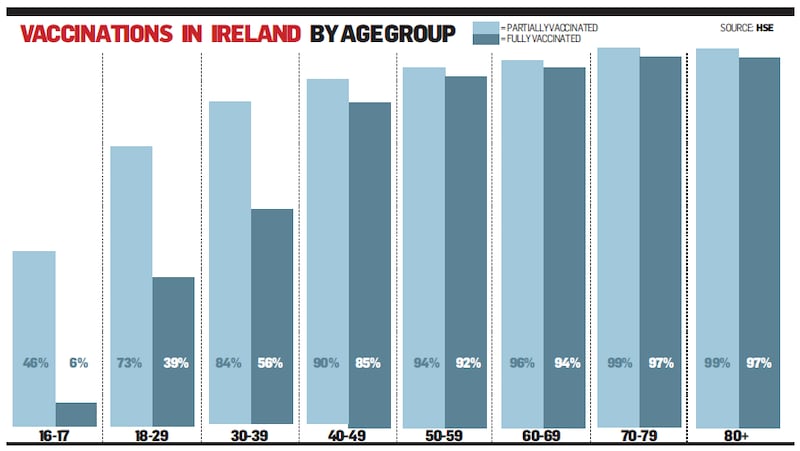
Well over four billion doses of Covid-19 vaccine have been administered worldwide since the end of 2020. The products developed have proved to be highly effective and safe. In Ireland, this and the high levels of trust in public health officials have seen our vaccine take-up soar to a very high level; almost 90 per cent of the adult population have had at least one dose.
Side-effects reported
Inevitably with such high numbers there have been reports of side-effects. One issue relates to very rare cases of myocarditis and pericarditis (heart-related inflammation) with a higher than expected rate reported in the US, predominantly among men aged 30 years and under. There, the highest reporting rate has been in males aged 12-17 years – more or less the current age-group being targeted for immunisation in Ireland.
According to Niac, most cases are self-limited and resolve with treatment of symptoms, though it adds that follow-up will be needed to determine whether there are longer-term effects.
“Data on the incidence of these events in children and young people are currently limited, and the longer-term health effects from the myocarditis events reported are not yet well-understood,” the JCVI concluded in the UK.
In Ireland, there have been 17 reports linked to myocarditis/pericarditis, but none among children. The youngest report concerned a patient aged 38.
In such a fast-moving situation, it is not possible to set out a detailed risk/benefit analysis for Covid-19 vaccines in children, though clearly the equation is evenly balanced.
Niac also took into account the indirect benefits of vaccination, particularly in light of the spread of the Delta variant. While not the primary drivers of transmission of the disease, in households or elsewhere, children do contribute to spread. Their vaccination, it is hoped, will reduce the amount of onward transmission.
In its decision, Niac cited a recent study which found that adults vaccinated with the Pfizer vaccine and who were later infected were up to 50 per cent less likely to transmit the virus in a household setting.
However, the US Centers for Disease Control has made the point recently that even fully vaccinated people can transmit the virus.
Niac based its decision in favour of vaccinating 12-15 year olds on criteria wider than indirect medical benefit. “In the unique circumstances of the pandemic, consideration regarding recommending Covid-19 vaccination to this age cohort must extend to include their physical, psychological and social wellbeing.”
‘Normalisation of life’
Universal vaccination of adolescents offers direct and indirect benefits, such as reducing the risk of severe disease, keeping schools open and "facilitating psychosocial development", it found.
“The primary benefits of vaccinating healthy 12-15 year olds will be normalisation of life, less disruption to educational and social activities, and reduced virus transmission to vulnerable household contacts.”
These conclusions were reached after holding focus group meetings with parents and young people. “There was an expectation that vaccination might be a step toward getting life back to normal and might facilitate more freedoms in terms of school and social activities,” the research found.
Relying on unpublished focus group studies reporting a yearning for a return to normal life doesn’t feel like “following the science”. Yet this research appears to have tipped the balance in favour of universal vaccination of young people.
Niac has also argued that universal vaccination of young people may impede the development of new variants that could lead to the development of severe disease in adolescents.
Early vaccination of healthcare workers and other vulnerable adults in developing countries would probably do more to prevent the emergence of new variants than vaccinating low-risk children in Ireland and other wealthy nations.
The World Health Organisation has suggested a pause on booster vaccinations until supplies are provided to immunise 10 per cent of the world's population. Others have questioned the morality of western countries racing to vaccinate entire populations when coverage is so scant elsewhere.
There is a good case for Ireland using up the doses it has to hand or has ordered, but the 700,000 doses we plan to buy from Romania are supplies that could be used to help poor countries with little or no protection against the Delta variant.
Beyond the binary decision whether to vaccinate or not, some parents may opt to wait and see.
Will the current surge of cases abate soon or continue to grow? Will the Delta variant be shown to be more dangerous than previous strains? Can the concerns about rare reports of side-effects among vaccinated young people be adequately addressed?
Few of the big questions can be answered definitively or permanently, when the data is evolving so quickly.










